


This brief examines the frequency with which contraceptive care clients with clinical indications for sexually transmitted infections (STIs) do not receive appropriate testing during their visits—representing a missed opportunity for detection and treatment. We find that:
- One in three sexually active contraceptive care clients had a clinical indication for STI testing. Among these, one in four did not receive the recommended testing.
- Missed opportunities for STI testing were more likely among adolescents and older clients, non-Hispanic White clients, those who are married or cohabitating, and those without children.
- Receiving patient-centered contraceptive care did not significantly reduce the likelihood of experiencing a missed opportunity for STI testing.
Introduction
Sexually transmitted infections (STIs) have become an increasing concern—particularly for women and girls, who’ve experienced disproportionately high rates of (and increases in) STI incidences over the last decade or more. Although recent efforts have been somewhat successful in bringing down some infection rates (e.g., gonorrhea declined by 14.1% and chlamydia decreased by 1.7% among women in 2023), disparities between females and males still exist. For example, 2023 data on STI cases by sex suggest that the chlamydia rate is almost twice as high among female patients (610.7 per 100,000) as among males (368.3)—a disparity especially pronounced among adolescents, with 2,566.1 per 100,000 cases among females ages 15-19 and 886.1 among males of the same age. Similarly, rates of primary and secondary syphilis increased by 107.7 percent from 2019 to 2023 among women, compared to an increase of 18.0 percent among men.
These rates are especially concerning given that untreated STIs have lifelong reproductive health consequences, including the risk of congenital syphilis, chronic pain, high-risk pregnancies, cancer, and infertility. To address this trend, the Centers for Disease Control and Prevention (CDC) has prioritized STI screening specifically among sexually active young women for 2022-2026.
We know that, for various reasons, many people do not receive STI care; barriers include affordability, limited appointment availability, transportation, geographic location, and inadequate provider training, among others. For those able to navigate these barriers and obtain a family planning appointment, it is essential to provide comprehensive care that minimizes their need for repeat visits. Building on CDC’s priorities to increase STI screening, sexual and reproductive health experts have called for greater integration of STI testing within family planning settings, which offer contraceptive, pregnancy, infertility, and preconception care, as well as STI testing and counseling. The 2024 national recommendations for Quality Family Planning (QFP) services emphasize STI and HIV prevention, screening, and treatment as essential components of high-quality sexual and reproductive health care. These guidelines encourage family planning providers to gather a full and accurate sexual history and incorporate counseling, screening, and treatment into routine care.
However, integrating STI testing into family planning care has not always been standard. For decades, researchers have debated whether this approach is effective for reaching those in need of STI services. They argue that key populations for STI testing (namely men and young people) do not frequently use family planning services. Additionally, concerns have been raised about the cost-effectiveness of investing in diagnostic technologies, given the relatively low number of STI cases family planning clinics might detect.
Research on STI testing in the context of contraceptive care remains limited, with most existing studies focusing on adolescents and young adults. These studies reveal significant variability in the rates at which family planning patients receive STI testing. The likelihood of receiving STI testing differs by type of contraceptive method sought, type of family planning appointment, and clients’ race/ethnicity.
About this brief
The analysis presented in this brief aims to provide updated estimates of how often sexually active contraceptive care clients with clinical indications for STI testing did not receive testing, representing missed opportunities for testing within contraceptive care. Specifically, we examine demographic characteristics and visit-related factors, such as method of payment and facility type, to document where potential intervention points may exist. Additionally, we examine the relationship between clients’ experiences of patient-centered contraceptive care[1] and missed opportunities for STI testing. While this measure is specifically designed to assess providers’ approach to contraceptive counseling rather than STI care, there are no equivalent patient-centered STI care measures available. However, patient-centered contraceptive care has been shown effective in improving care outcomes, suggesting that it may also enhance STI care outcomes in similar contexts. We include this measure to explore how providers’ approach to care delivery might better support the integration of STI testing into family planning services.
Our findings highlight critical gaps in care and underscore the importance of developing strategies to ensure the effective integration of STI testing into family planning services.
Methods
We pooled data from the 2015-2017 and 2017-2019 waves of the National Survey of Family Growth (NSFG)[2] female respondent files, which contain data on family planning and contraceptive care visits in the 12 months prior to interview. We limited our sample to contraceptive clients, who are those who indicated receiving birth control counseling or a medical test or checkup related to birth control in the past 12 months (N = 2,670). Clients whose contraceptive care only involved obtaining a method of contraception, without any counseling or medical tests, were excluded, as they may have simply picked up a method from a pharmacy and would not have been in the position to receive STI testing. We then created a subset of contraceptive clients who had reasons to test for STIs. These were contraceptive clients who had had intercourse in the past 12 months, as well as experiences that suggest a medical reason to receive STI testing,[3] per the CDC’s guidelines (N = 988). We refer to this subset of contraceptive clients as those with “reasons to test.” Details on statistical tests run for this analysis can be found in the methodological appendix.
Results
Of the sexually active NSFG respondents who had received contraceptive care in the last year, 35 percent (N = 988) had clinical indications for STI testing based on CDC guidelines (Figure 1). The most common experiences warranting testing among contraceptive clients included having had two or more sexual partners in the last year (19%), a history of past STIs (16%), and having a non-monogamous partner (14%). Less than 5 percent reported using illicit substances, having a partner who used IV drugs, or engaging in transactional sex in the past year.
Of these contraceptive care clients with a reason to receive STI testing, half were ages 20-29, over half (63%) identified as non-Hispanic White, 60 percent had no children, and just under half (48%) had incomes at or above 250 percent of the federal poverty level. Most of these clients were neither married nor living with a partner (71%), identified as straight or heterosexual (80%), and lived in an urban area (87%). We also considered the characteristics of the contraceptive care these clients received. Twenty-eight percent received publicly funded contraceptive care (Medicaid or free services) and about one quarter received care at a Title-X facility (14%) or another publicly funded facility (10%).
Figure 1. More than one in four contraceptive clients whose experiences warranted STI testing didn’t receive it
Proportion of contraceptive clients with experiences that warrant STI testing and proportion who didn’t receive testing
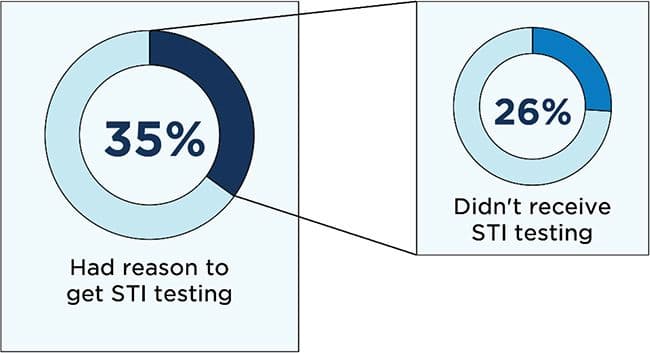
Source: NSFG Female Respondent Files, 2015-2017 and 2017-2019
Without accounting for other demographic characteristics, non-Hispanic Black clients and unmarried clients not living with a partner were less likely than their counterparts to experience a missed opportunity for STI testing. Conversely, clients ages 15-19 and those who received their contraceptive care at a private facility had higher odds of missing an opportunity for testing.
Figure 2 displays results from analyses[4] testing of the association between missed opportunities for testing and demographic and contraceptive care characteristics. When adjusting for demographic and care-related characteristics, we found that age was significantly associated with missed opportunities. Compared to individuals ages 20–29 (reference group), adolescents ages 15–19 (adjusted odds ratio [aOR]: 2.96, p = 0.002), adults ages 30–39 (aOR: 1.75, p = 0.040), and those ages 40+ (aOR: 3.83, p < 0.001) had a consistently higher likelihood of missed opportunities for STI testing.
Race and ethnicity were also consistently associated with missed opportunities: Black, non-Hispanic individuals were significantly less likely to experience missed opportunities than their White, non-Hispanic counterparts (aOR: 0.54, p = 0.018).
Similarly, patients’ relationship status and number of children were strong predictors of missed opportunities. Married individuals had significantly higher odds of missed opportunities (aOR: 3.15, p < 0.001), as did those cohabiting (aOR: 2.28, p = 0.010), relative to individuals who were not married or cohabiting. Additionally, having more children was associated with lower odds of missed opportunities. Individuals with three or more children were about 25 percent less likely to experience a missed opportunity for testing than those with no children (aOR: 0.27, p = 0.003).
We ran three different tests to determine the role of different contraceptive care characteristics in the likelihood of experiencing a missed opportunity for testing. First, we found that receiving care at a private facility was marginally associated with higher odds of a missed opportunity (aOR: 2.48, p = 0.115), relative to those who had received care at Title X facilities. Additionally, we found that patient-centered care was also marginally associated with reduced odds of missed opportunities (aOR: 0.56, p = 0.069). Those who received publicly funded care (Medicaid or free care) were no more or less likely to experience a missed opportunity for testing than those who did not.
Finally, we examined contraceptive clients’ main reported reasons for not getting STI testing in the last year. We found that 40 percent with reason to test indicated that their doctor did not offer or ask them about STI testing. Fifty percent reported “other” reasons[5] for not getting tested.
Figure 2. Married and cohabitating patients, older and younger patients, and non-Hispanic White patients were more likely to have missed opportunities for STI testing
Patient and care characteristics associated with higher and lower likelihood of having a missed opportunity for testing
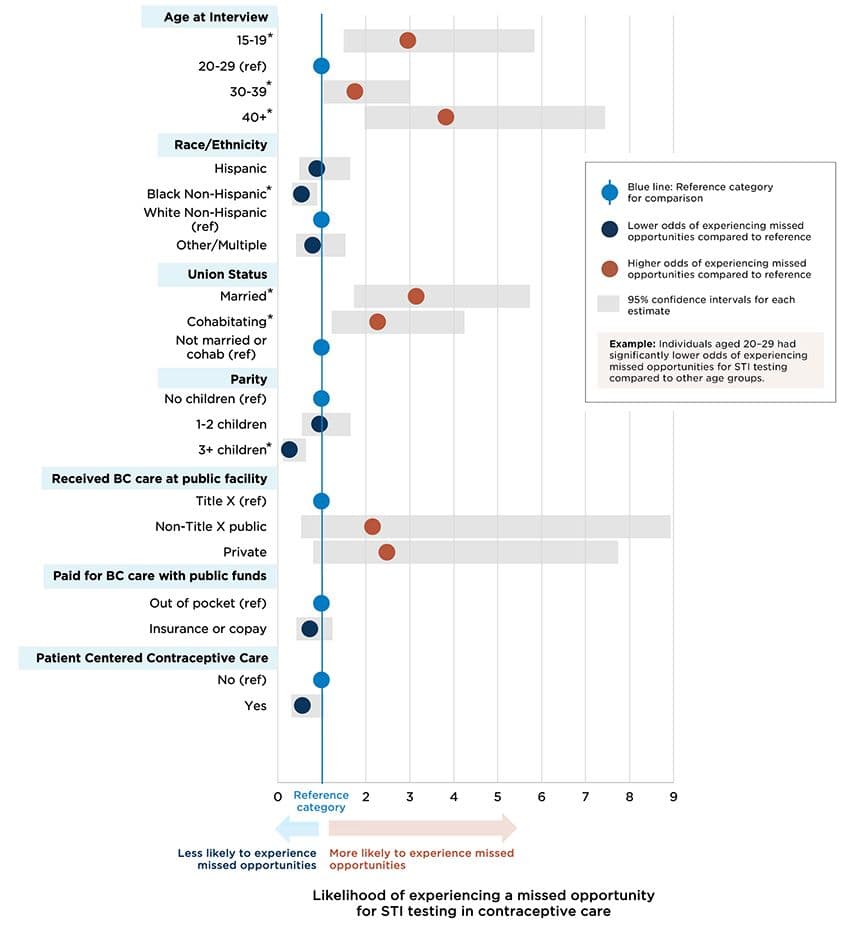
* Asterisks represent groups with a significantly different (higher or lower) odds of missed opportunities compared to the reference group.
Source: NSFG Female Respondent Files, 2015-2017 and 2017-2019
Discussion and Recommendations
Despite decades of discourse on integrating STI testing into family planning care, our findings reveal persistent missed opportunities for testing among sexually active contraceptive care clients. In fact, our analysis found that one in three contraceptive care clients had clinical reasons to receive STI testing based on CDC guidelines, but over 25 percent of those did not receive this care. These gaps in care are especially concerning given rising STI rates and the persistent barriers many individuals face in accessing timely testing and treatment.
The most common reason patients cited for not getting STI testing was that their providers did not offer it, underscoring gaps in clinical protocols and provider-patient communication. Adolescent-centered approaches to taking sexual history, such as indirect questioning, can help identify the need for STI testing and foster more open conversations. Indirect questioning involves asking broader, less intrusive questions rather than directly inquiring about behaviors, a practice that helps adolescents feel more comfortable sharing sensitive information. Similarly, allowing time for patient questions and fostering patient participation may facilitate more effective sexual health conversations. Additionally, a notable proportion of respondents listed “other” reasons for not being tested, suggesting the need for further qualitative research to unpack the nature of these barriers. Existing research has pointed to factors such as confidentiality concerns among adolescents and rural residents, perceived STI stigma and fear of judgement, and assumptions of low likelihood of STI exposure as being influences on patients’ decisions to pursue (or not pursue) testing.
Missed opportunities for STI testing did not equally affect all demographic groups. Non-Hispanic White clients were more likely to experience missed opportunities than their non-Hispanic Black counterparts. While low rates of missed opportunities among non-Hispanic Black women might seem like a result worth celebrating, this finding warrants deeper exploration. Research suggests that racial stereotypes, such as the hyper-sexualization of Black women, may inadvertently lead providers to assume higher likelihood of STI exposure among certain groups, resulting in disparate testing practices. These assumptions may also increase the likelihood of unfair treatment during care, which other Child Trends research suggests is prevalent in family planning settings.
Similarly, we observed higher rates of missed opportunities among married or cohabitating clients, possibly reflecting provider biases that equate marital status with monogamy and lower likelihood of STI exposure. However, all clients in our sample, including the married ones, had clinical reasons for testing. Providers must avoid assumptions about sexual behavior based on marital status and instead focus on thorough assessments based on patients’ actual (versus presumed) behaviors.
Patient-centered contraceptive care was not significantly associated with a reduced likelihood of missed opportunities for STI testing. While patient-centered contraceptive care is associated with positive outcomes in contraception counseling and other reproductive health services, it was not developed with the goal of improving STI-related care. Its limited relationship with STI testing, while not necessarily unexpected, underscores a critical gap in care models that aim to integrate STI services within family planning care. This finding highlights the need to develop patient-centered comprehensive care models that explicitly address STI screening and counseling to ensure that health care providers can deliver unbiased and respectful care. Leveraging tools and resources—like the National Coalition for Sexual Health’s Sexual Health Questions to Ask All Patients—offer promising avenues to help normalize comprehensive sexual health conversations, including STI testing within the broader context of family planning care.
Our findings also highlight the influence of health care system factors on missed opportunities. Publicly funded facilities, such as Title X-funded clinics, often adhere to best practices for STI screening, as outlined in the newly updated guidance on the provision of Quality Family Planning. This adherence likely contributes to higher testing rates compared to private facilities. While the association between receiving care in a public facility and lower missed opportunity rates was not statistically significant after adjusting for demographics, the trend remains noteworthy: It suggests that public facilities may be better aligned with evidence-based practices. Additionally, we found that method of payment was also not associated with missed opportunities, indicating that cost alone may not be the primary barrier to testing in these settings. Instead, these findings suggest that demographic factors are stronger predictors of disparities in STI testing, which may in turn reflect provider biases in implementing testing protocols.
Recommendations
To reduce missed opportunities for STI testing in family planning care, we recommend several programmatic and policy changes:
- Implement opt-out testing models. Opt-out approaches for STI testing, as recommended in the QFP guidelines, could normalize testing, decrease stigma, and reduce reliance on provider discretion.
- Offer training to providers. All clinic staff should receive training on gathering a full and accurate sexual history, assumptions they may make about patients, and proper billing and coding practices to ensure consistent care while maximizing reimbursement.
- Integrate person-centered tools. Incorporating counseling frameworks that seamlessly incorporate gathering a full and accurate sexual history and testing into patient-centered contraceptive are models that could enhance patient outcomes and address care gaps.
- Translate best practices from public facilities to private care settings. Public health facilities, particularly Title X clinics, often achieve higher testing rates due to robust policies. Identifying ways to adapt these best practices for private care settings, including financial incentives and structural support, could improve STI testing rates and care consistency across the health care system.
Additional research should be conducted on the following:
- Investigate providers' experiences and challenges, particularly those in private care settings, when integrating STI testing into contraceptive care.
- Examine strategies to seamlessly incorporate routine STI testing into contraceptive care models, including approaches like proactive provider-initiated testing and opt-out testing frameworks.
- Disaggregate the types of STI testing collected in research: Understanding rates of gonorrhea and chlamydia testing compared to syphilis testing is crucial to tailoring STI interventions.
We conducted a series of analyses for this brief. First, we ran tabulations to examine the prevalence of experiences that suggest clinical reasons to test for STIs among sexually active contraceptive care clients, followed by crosstabulations to determine rates of missed opportunities among those with each of these experiences. Next, we produced frequencies of demographic and family planning health care characteristics of those with reasons to test and performed chi-square tests to determine whether there are demographic differences between those who had a missed opportunity for testing and those who didn’t.
To understand the factors associated with a higher likelihood of missed opportunities, we first ran bivariate and then multivariate logistic regressions to assess the relationship between individuals’ demographic and SRH characteristics and missed opportunities. Variables were included in the multivariate models if they were significant at the bivariate level (p ≤ 0.05).
With a smaller sample of contraceptive clients from the 2017-2019 NSFG, in which additional variables were available, we explored the association between patient-centered contraceptive care and missed opportunities for STI testing. We also examined explanations reported by clients within this smaller sample who had reasons to test if they did not receive testing.
Acknowledgements
The authors wish to thank Elizabeth Quinteros, Catherine Schaefer, and Kate Welti for reviewing drafts and providing feedback throughout its development, and Catherine Nicols for designing our data visualizations.
This publication was made possible by cooperative agreement CDC-RFA-PS-23-0007 from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention (CDC).
Footnotes
[1] Patient-centered contraceptive care is the new “gold standard” for contraceptive care delivery and is measured with four survey questions asking patients to rate their providers. More information can be found here: https://pcccmeasure.ucsf.edu/
[2] The NSFG is a nationally representative survey collected by HHS of people ages 15-49.
[3] Reasons include past experience with STIs; use of intravenous drugs, cocaine, methamphetamine, or crack cocaine in the past 12 months; more than one sexual partner, or a partner with more than one sexual partner in the past 12 months; a sexual partner who used intravenous drugs in the past 12 months; or transactional sex in the past 12 months.
[4] We conducted multivariate logistic regressions, controlling for age, race/ethnicity, marital status, parity, facility type where the client received contraceptive care, client’s method of payment for contraceptive care, and client’s receipt of patient-centered contraceptive care.
[5] Response options provided for this question in the NSFG (WHYNOSTD) include: didn't want parents to find out, concerned about confidentiality, embarrassed or difficult to ask to be tested, cost or lack of insurance, other, refused, and don’t know, in addition to doctor or health care provider never suggesting testing. Respondents are asked to select from these options the one main reason why they had not been tested for a sexually transmitted disease in the past 12 months. This question was only asked in the 2017-2019 wave of the NSFG. We use pooled 2015-2019 data for this brief, so these results reflect responses for only half of the sample.
Suggested citation
Pliskin, E., & Rogers, J. (2025). Missed opportunities for STI testing in contraceptive care. Child Trends. DOI: 10.56417/5413s7247p