



In recent years, New York State and Washington, DC have enacted policies granting paid time off to workers seeking prenatal care or other pregnancy-related medical care. These policies offer workers job protection and allow them to receive their full income when taking time off to receive care. Both New York and Washington, DC supplement existing paid family leave policies that workers can use during the postpartum period, meaning that workers can use this paid leave to attend critical prenatal visits without impacting the length of leave they can take once their babies are born.
Timely and regular prenatal care provides an opportunity to identify and manage potential complications for both pregnant people and fetuses during pregnancy, including infection, gestational diabetes, preeclampsia, mental health concerns, substance use, and genetic conditions or other fetal abnormalities. Prenatal care visits also provide an opportunity to screen patients for risk factors like stress, unstable housing, and intimate partner violence, and to provide referrals for resources and education on topics related to pregnancy and neonatal health. Receipt of prenatal care is associated with lower risk of adverse outcomes such as low birthweight, preterm birth, infant mortality, and maternal mortality.
Despite this importance, in 2023, 7 percent of women who gave birth in the United States received late (beginning in the third trimester) or no prenatal care, according to data from the National Vital Statistics System. This is slightly higher than the previous year (6.8%) and the highest percentage reported in the years for which we have national data on this topic (2016-2023).
Figure 1. The percentage of women receiving late or no prenatal care has risen substantially since 2021
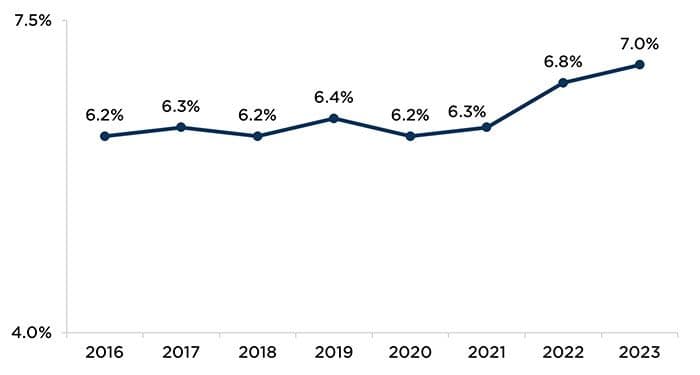
Source: Osterman, M., Hamilton, B., Martin, J., Driscoll, A., & Valenzuela, C. (2025). Births: Final data for 2023. National Vital Statistics System. https://www.cdc.gov/nchs/data/nvsr/nvsr74/nvsr74-1.pdf
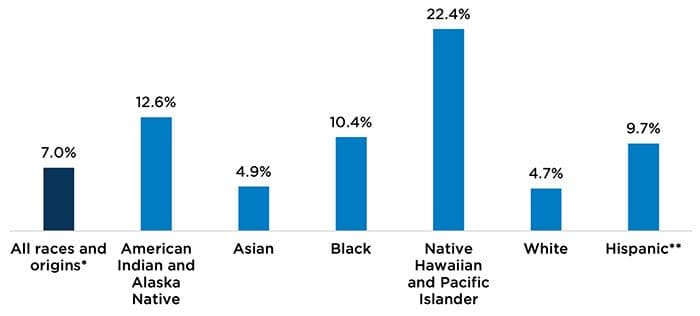
These same data indicate that receipt of timely prenatal care in 2023 varied significantly by women’s race and ethnicity. White and Asian women were less likely to receive late or no prenatal care than their counterparts of other races and ethnicities (Figure 2).
Figure 2. Receipt of late or no prenatal care varies by women’s race/ethnicity (2023)
Source: Osterman, M., Hamilton, B., Martin, J., Driscoll, A., & Valenzuela, C. (2025). Births: Final data for 2023. National Vital Statistics System. https://www.cdc.gov/nchs/data/nvsr/nvsr74/nvsr74-1.pdf
Note: “Late” care refers to care initiated in the third trimester of pregnancy.
* Includes births to race and origin groups not shown separately, including Hispanic single-race Black, Hispanic single-race White, and non-Hispanic multiple-race women, in addition to births for which race/origin group is not stated.
** Includes people of Hispanic origin of any race.
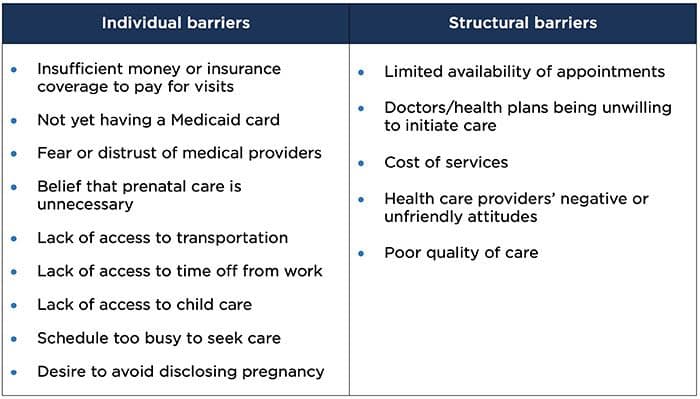
Delays in accessing timely prenatal care may be attributed to a range of intersecting individual and structural barriers pregnant people face (Table 1). Policies like those in New York and Washington, DC are intended to make it easier for more people to access this care by removing some of these barriers. While these policies have yet to be comprehensively evaluated, they are a promising step toward supporting the health and economic well-being of pregnant workers and their families.
Table 1. Barriers to accessing timely prenatal care
Sources: Krukowski, R., Jacobson, L., John, J., Kinser, P., Campbell, K., Ledoux, T., Gavin, K., Chiu, C., Wang, J., & Kruper, A. (2021). Correlates of early prenatal care access among U.S. women: Data from the Pregnancy Risk Assessment Monitoring System (PRAMS). Maternal and Child Health Journal. 26, 328-341. https://doi.org/10.1007/s10995-021-03232-1; Testa, A., Lee, J., Semenza, D., Jackson, D., Ganson, K., & Nagata, J. (2023). Intimate partner violence and barriers to prenatal care. Social Science and Medicine. 320(March 2023). https://doi.org/10.1016/j.socscimed.2023.115700; Phillipi, J. (2009) Women’s perceptions of access to prenatal care in the United States: A literature review. Journal of Midwifery & Women’s Health. May-June; 54(3): 219-25. https://doi.org/10.1016/j.jmwh.2009.01.002; Testa, A., & Jackson, D. (2021). Barriers to prenatal care among food-insufficient women: Finding from the Pregnancy Risk Assessment Monitoring System. Journal of Women’s Health. 30(9). https://doi.org/10.1089/jwh.2020.8712
Child Trends has developed a Guide to Evaluating Paid Family and Medical Leave Policies to help states and localities assess whether their policies, including policies targeting prenatal leave, are achieving their intended outcomes. If you are interested in learning more about this guide, or in working with us on evaluating paid family and medical leave policies, please contact Kate Steber, Katy Falletta, or Julianna Carlson.
Suggested citation
Falletta, K., Steber, K., & Carlson, J. (2025). New state paid leave policies grant parents access to critical prenatal care. Child Trends. DOI: 10.56417/1384b6600a