%202-800x800.jpg&w=3840&q=75)

A growing body of research has made it increasingly apparent that adverse childhood experiences (ACEs) are a critical public health issue. ACEs are potentially traumatic experiences and events, ranging from abuse and neglect to living with an adult with a mental illness. They can have negative, lasting effects on health and well-being in childhood or later in life.1 However, more important than exposure to any specific event of this type is the accumulation of multiple adversities during childhood, which is associated with especially deleterious effects on development.2
There is growing interest in understanding the prevalence of these experiences across different communities in the United States, and how to prevent and respond to them. One mechanism responsible for these effects—toxic levels of stress—can be substantially buffered by a stable and supportive relationship with a caregiver.
This brief uses data from the 2016 National Survey of Children’s Health (NSCH) to describe the prevalence of one or more ACEs among children from birth through age 17, as reported by a parent or guardian. The data are representative at national and state levels. The study team estimated the national prevalence of eight specific ACEs and compared the prevalence of these ACEs across states. To examine prevalence differences by race/ethnicity and geography, we used the nine geographic divisions used by the U.S. Census Bureau.3
Key Findings
- Economic hardship and divorce or separation of a parent or guardian are the most common ACEs reported nationally, and in all states.
- Just under half (45 percent) of children in the United States have experienced at least one ACE, which is similar to the rate of exposure found in a 2011/2012 survey.* In Arkansas, the state with the highest prevalence, 56 percent of children have experienced at least one ACE.
- One in ten children nationally has experienced three or more ACEs, placing them in a category of especially high risk. In five states—Arizona, Arkansas, Montana, New Mexico, and Ohio—as many as one in seven children had experienced three or more ACEs.
- Children of different races and ethnicities do not experience ACEs equally. Nationally, 61 percent of black non-Hispanic children and 51 percent of Hispanic children have experienced at least one ACE, compared with 40 percent of white non-Hispanic children and only 23 percent of Asian non-Hispanic children. In every region, the prevalence of ACEs is lowest among Asian non-Hispanic children and, in most regions, is highest among black non-Hispanic children.
* Child Trends reported on these data in an earlier publication: Adverse Childhood Experiences: National and State-level Prevalence. The Health Resources and Services Administration’s Maternal and Child Health Bureau and the Child and Adolescent Health Measurement Initiative’s Data Resource Center caution against making direct comparisons of 2016 data with those collected in earlier waves of the survey, because of design changes in 2016.
ACEs can cause stress reactions in children, including feelings of intense fear, terror, and helplessness. When activated repeatedly or over a prolonged period of time (especially in the absence of protective factors), toxic levels of stress hormones can interrupt normal physical and mental development and can even change the brain’s architecture. ACEs have been linked to numerous negative outcomes in adulthood, and research has increasingly identified effects of ACEs in childhood.4,5 Negative outcomes associated with ACEs include some of society’s most intractable (and, in many cases, growing) health issues: alcoholism, drug abuse, depression, suicide, poor physical health, and obesity. There is also some evidence that ACEs are linked to lower educational attainment, unemployment, and poverty.6 In childhood, children who have experienced ACEs are more likely to struggle in school and have emotional and behavioral challenges.7 Nevertheless, not all children who experience one of these adverse events (or even more than one) are negatively affected; much depends on the context in which they occur—particularly the context of positive relationships.
Research has found that the risk for negative outcomes increases with the number of ACEs; in other words, children who have experienced multiple ACEs are substantially more likely to be negatively affected than children who have experienced only one.8,9 A seminal study published in the late 1990s by Felitti, Anda, and their colleagues (that first coined the term “adverse childhood experiences”) found that adults who had experienced four or more ACES had a particularly high risk for negative physical and mental health outcomes, including some of the leading causes of death in the United States.10 Subsequent studies have identified lower thresholds, ranging from one to three ACEs, as the tipping point at which risk increases greatly.11,12 There are likely to be multiple factors that account for individual variation in response to adversity, including genetic predispositions and other biological characteristics, as well as contextual factors such as supportive adult relationships.
One of the most sobering findings regarding ACEs is preliminary evidence that their negative effects can be transmitted from one generation to the next.13,14 Toxic stress experienced by women during pregnancy can negatively affect genetic “programming” during fetal development, which can contribute to a host of bad outcomes, sometimes much later in life.15 Infants born to women who experienced four or more childhood adversities were two to five times more likely to have poor physical and emotional health outcomes by 18 months of age, according to one recently published study.16
Measurement of Adverse Childhood Experiences
There is no single agreed-upon list of experiences that encompass what we refer to as adverse childhood experiences. The original ACEs study asked a large sample of adults about seven childhood experiences: psychological, physical, and sexual abuse, as well as exposure in the home to substance abuse, mental illness and suicide, incarceration, or violence.17 Since then, the list of ACEs used in one or more studies has been expanded to include physical and emotional neglect, parental separation and divorce, exposure to violence outside of the home, living in unsafe neighborhoods, homelessness, bullying, discrimination based on race or ethnicity, and experience of income insecurity.18 One reason for the development of different ACEs measures that incorporate a broader set of experiences is that researchers and practitioners have sought to better capture the diverse experiences of children from different backgrounds, particularly children of color and those living in poverty. However, no list is likely to include all adversities and traumatic experiences that children may experience. Thus, researchers and practitioners should be aware that screening for ACEs does not substitute for comprehensive trauma screening and assessment, for which there are many well-validated tools.19
The 2016 NSCH includes nine ACEs; we report here on the prevalence of eight of those experiences.* The biggest difference between the list of ACEs in the NSCH data and other lists used in the research (or as part of the screening tools used to identify children with ACEs) is that the NSCH data do not explicitly ask parents to report on their child’s experiences of abuse and neglect. Specifically, parents are asked about whether their child has ever:
1. Lived with a parent or guardian who became divorced or separated
2. Lived with a parent or guardian who died
3. Lived with a parent or guardian who served time in jail or prison
4. Lived with anyone who was mentally ill or suicidal, or severely depressed for more than a couple of weeks
5. Lived with anyone who had a problem with alcohol or drug
6. Witnessed a parent, guardian, or other adult in the household behaving violently toward another (e.g., slapping, hitting, kicking, punching, or beating each other up)
7. Been the victim of violence or witnessed any violence in his or her neighborhood
8. Experienced economic hardship “somewhat often” or “very often” (i.e., the family found it hard to cover costs of food and housing)
* The ninth item that parents are asked to report on is how often their child was treated or judged unfairly because of his or her race or ethnicity. We do not include this ACE in this analysis, both because of the subjectivity of the question (what constitutes unfair treatment or judgement is open to different interpretations) and because parents may not be reliable reporters of their child’s experience in this area (for example, parents may not be aware of the extent of their child’s experiences of discrimination).
State-Level Variation in the Prevalence of Adverse Childhood Experiences
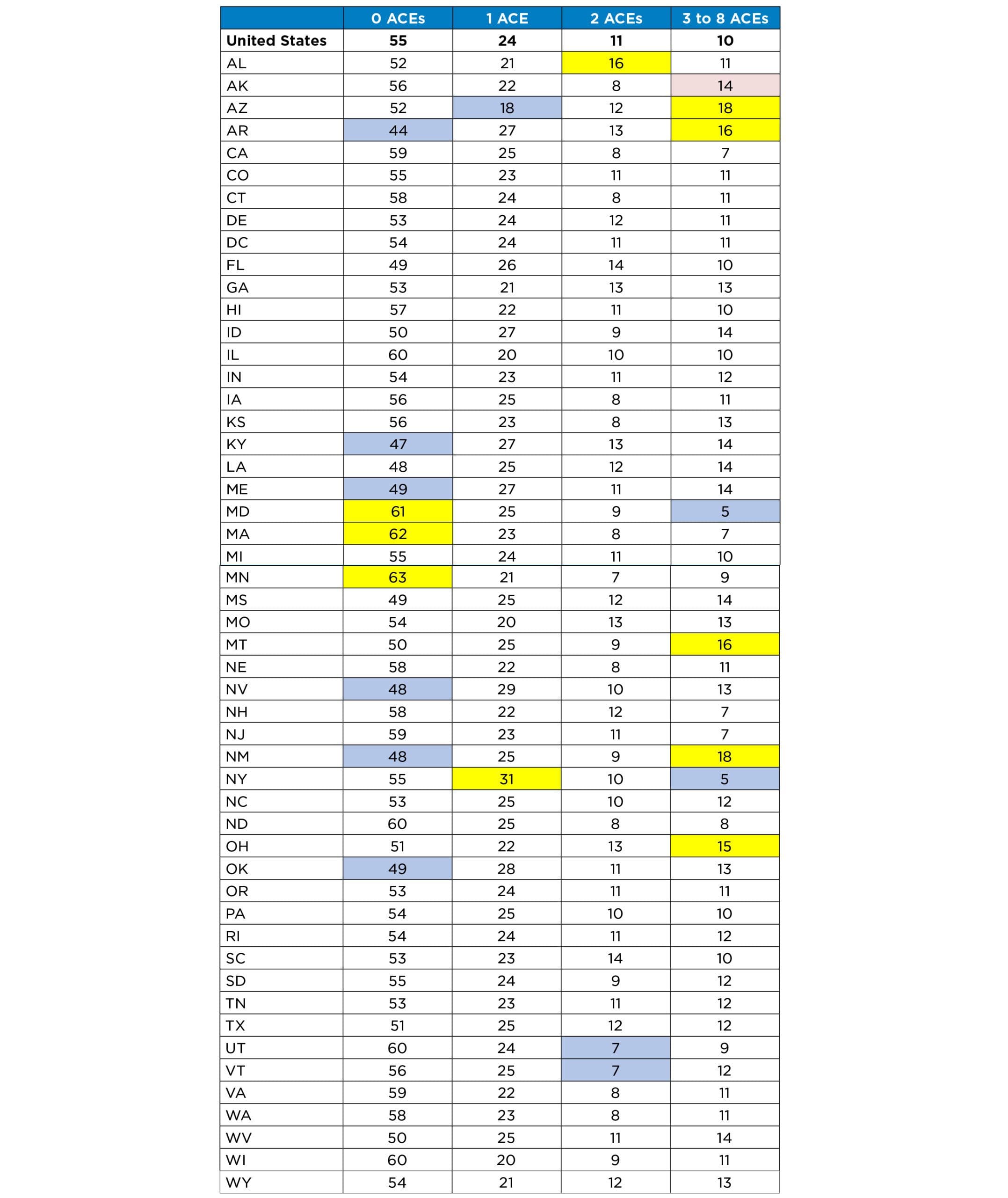
Table 1 shows the prevalence of one or more ACEs, according to parents’ reports on their child, both nationally and by state. Nationally, 55 percent of children had experienced no ACEs. The percentage of children who had experienced no ACEs was significantly higher than the national average in three states: Maryland, Massachusetts, and Minnesota. At the national level, about one in ten children (10 percent) had experienced three or more ACEs. In five states—Arizona, Arkansas, Montana, New Mexico, and Ohio—as many as one in seven children had experienced three or more ACEs, a significantly higher ratio than the national average.
Table 1. Among Children from Birth through Age 17, Percentage Reported to Have Had Zero, One, Two, and Three or More ACEs, Nationally and by State
Yellow shading = Percentage is higher than the national average at a statistically significant level.
Blue shading = Percentage is lower than the national average at a statistically significant level.
Red shading = Estimate should be interpreted with caution, because the relative confidence interval is greater than 120 percent. See the “About the data used in this report” section for more information.
Research indicates that several protective factors can prevent or ameliorate the negative effects of ACEs.26 A positive, supportive relationship with one or more adults is of primary importance.27 Studies show that children with secure attachment relationships with their caregiver(s) are better able to regulate their responses to upsetting situations, compared to children with less secure caregiver attachments.28 In addition to supportive relationships, a child’s own intrapersonal skills can be a buffer to the effects of ACEs. Children who have experienced ACEs but demonstrate adaptive behaviors, such as managing their emotions, are more likely to have positive outcomes.29 Children and adults alike can help cultivate resilience—for example, through practicing self-care routines and strengthening key social and emotional skills such as empathy, self-regulation, and self-efficacy.30
Another way to support resilience is the use of trauma-informed approaches when working with children, youth, and families. The growing interest in understanding ACEs has been accompanied by an increase in the development and application of trauma-informed care (TIC). TIC describes a variety of approaches that acknowledge the impact of trauma, recognize its symptoms, respond to its effects through appropriate practices and policies, and prevent further traumatization.31 Programs and organizations that use a trauma-informed approach may not necessarily treat the consequences of trauma directly, but instead train their staff to interact effectively with participants who have been affected. This may include supporting participants’ coping skills and use of appropriate behavior management techniques.32 TIC is increasingly used in systems and settings that involve young people and their families, including schools, the child welfare system, early child care and education settings, healthcare settings, and the juvenile justice system.33,34
Economic Hardship and Parental Separation or Divorce Are the Most Common Adverse Childhood Experiences
While the accumulation of ACEs, rather than any particular ACE, is most strongly predictive of negative outcomes, policymakers and practitioners will want to understand the specific challenges facing children in their own states, in order to target limited resources for relevant interventions. By the same token, efforts that reduce the likelihood that any single ACE will occur are likely to make a difference for overall well-being.
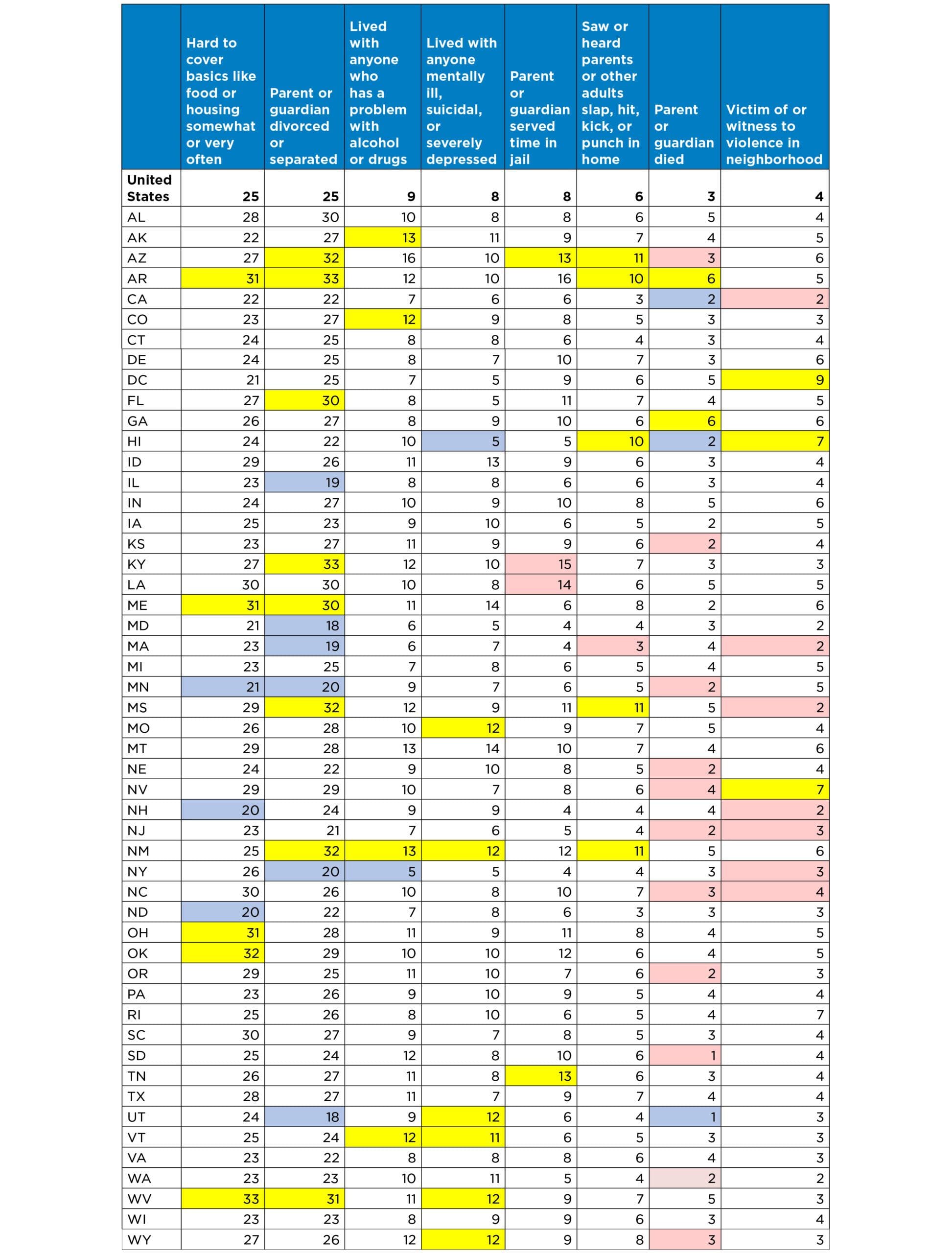
Nationally—and in all 50 states and the District of Columbia—the two most common ACEs are economic hardship and the separation or divorce of a parent or guardian. About one-quarter of children have experienced at least one of these events. In West Virginia, one in three children have experienced economic hardship, compared to a rate of just one in five in Minnesota, New Hampshire, and North Dakota. In Arkansas and Kentucky, about one-third of children have dealt with parental separation or divorce, just 18 to 19 percent have experienced the same in Illinois, Maryland, Massachusetts, and Utah.
Other ACEs—such as the death of a parent or guardian, or being the victim of or witnessing violence in the neighborhood—are more rare. Nationally, these experiences were identified for only three to four percent of children. However, these experiences are more common than the national average in a handful of states. For example, in Arkansas and Georgia, six percent of children have experienced the death of a parent or guardian. In Nevada and Hawaii, seven percent have been victims of, or have witnessed, violence in their neighborhood.
Table 2. Prevalence of Individual ACEs, Nationally and by State
Yellow shading = Percentage is higher from the national average at a statistically significant level.
Blue shading = Percentage is lower than the national average at a statistically significant level.
Red shading = Estimate should be interpreted with caution, because relative confidence interval is greater than 120 percent. See the “About the data used in this report” section for more information.
Disparities by Race and Ethnicity Are Evident at National and Regional Levels
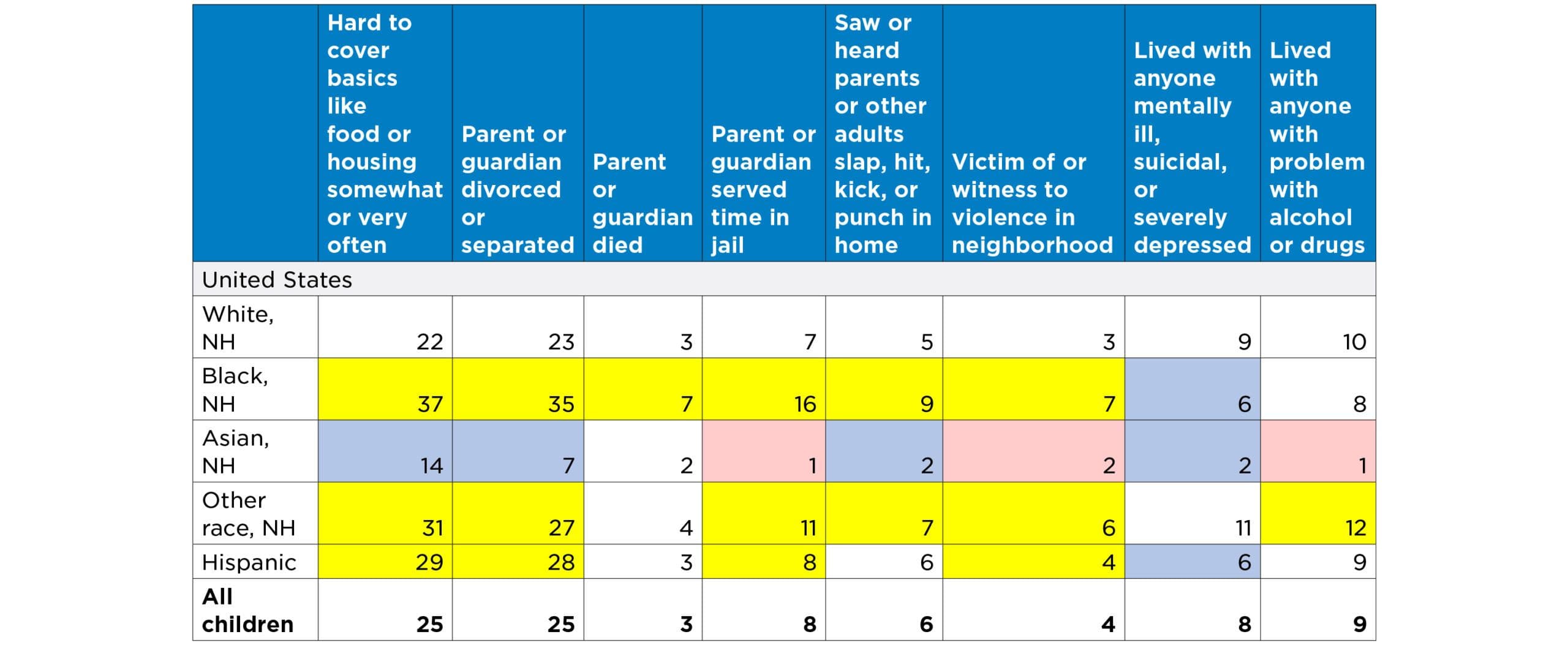
Table 3 shows the national prevalence of specific ACEs by racial and ethnic group.* Regardless of race/ethnicity, economic hardship and the divorce or separation of a parent or guardian are the most common ACEs reported for children. For white children, the next-most common experiences are living with an adult with mental illness, and living with an adult with a substance use problem. For black non-Hispanic children, parental incarceration is the next-most common ACE; for Hispanic children, the next-most common are living with an adult with a substance use problem and parental incarceration. Black non-Hispanic children are the most likely to have experienced the death of a parent or guardian.
* At the state level, estimates of children in specific racial and ethnic groups who experienced specific ACEs are often not reliable. Those figures are not presented here.
Table 3. Prevalence of Individual ACEs for Children in Various Racial/Ethnic Groups
Yellow shading = Percentage is higher than white non-Hispanic children at a statistically significant level.
Blue shading = Percentage is lower than white non-Hispanic children at a statistically significant level.
Red shading = Estimate should be interpreted with caution, because the relative confidence interval is greater than 120 percent. See the “About the data used in this report” section for more information.
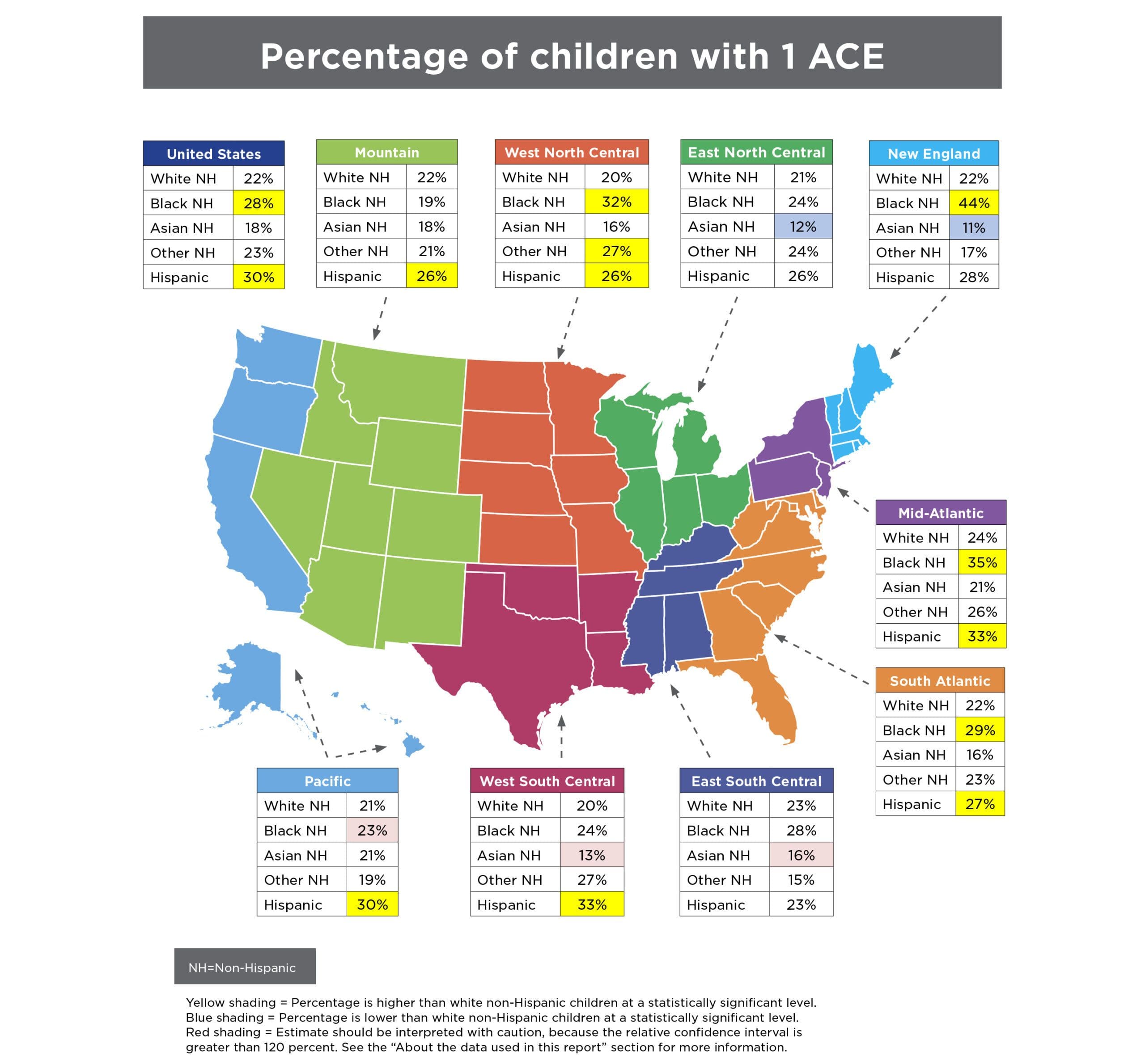
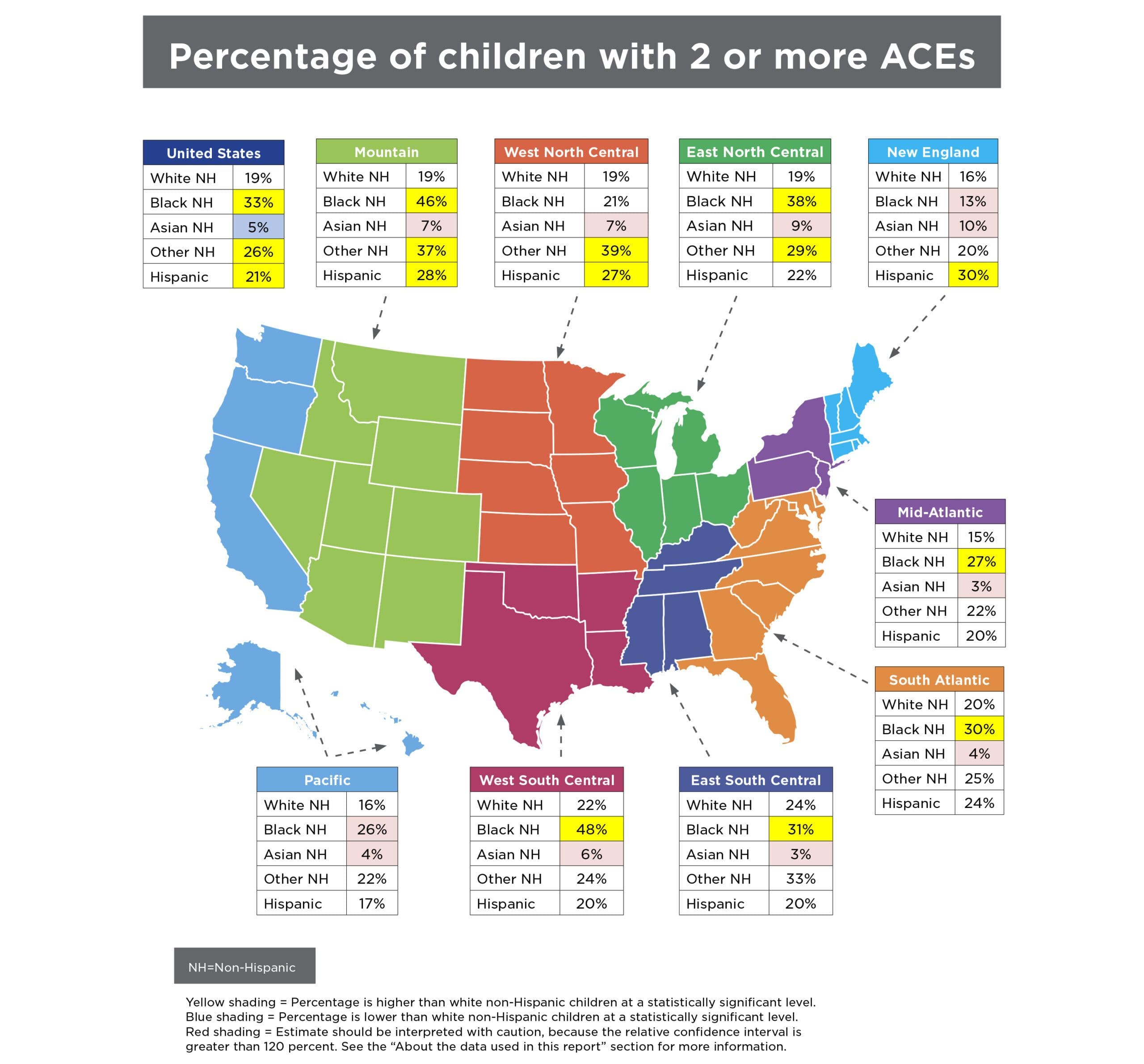
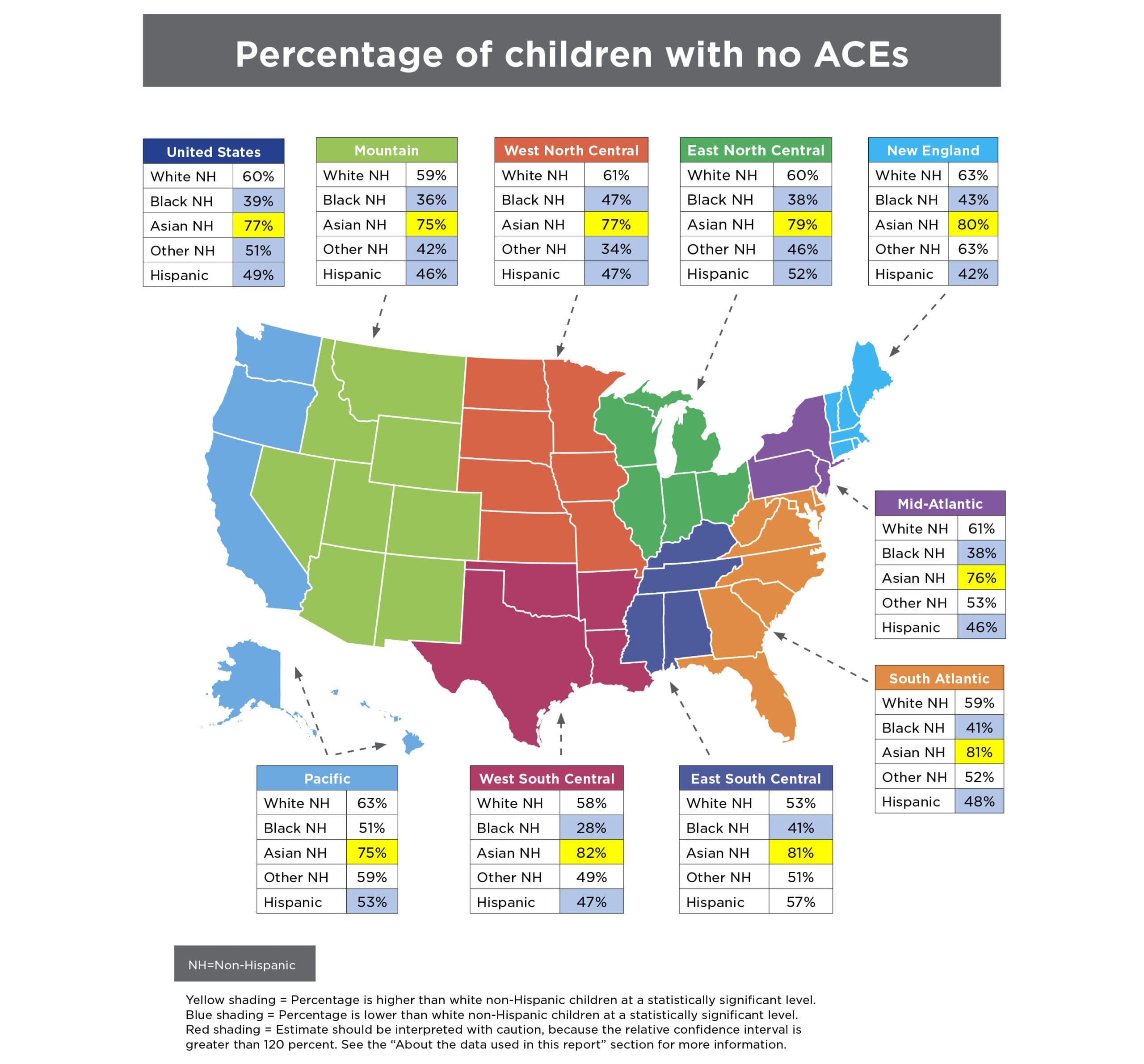
The overall risk for ACEs is not shared equally by all children. Whether the data are examined at the national level or by the country’s major geographic divisions, inequities by race and ethnicity are evident (see maps below). For example, at the national level, while 60 percent of white non-Hispanic children have had no ACEs, this is the case for only 49 percent of Hispanic children and 39 percent of black non-Hispanic children. In the United States as a whole and in every subregion, Asian non-Hispanic children have the lowest prevalence of ACEs—nationally, more than three-quarters of these children have had no ACEs. In every region except the Pacific, black non-Hispanic children are more likely than white non-Hispanic children to have had at least one ACE. In every region except the West South Central and the East South Central, Hispanic children are more likely than white non-Hispanic children to have had at least one ACE. Nationally, and in the Mountain region, black non-Hispanic children, non-Hispanic children of other races, and Hispanic children are more likely than white children to have experienced two or more ACEs. Nationally, one in three black non-Hispanic children have experienced two to eight ACEs, compared to only one in five white non-Hispanic children.
Addressing Adverse Childhood Experiences
Over the past several years, researchers, policymakers, and practitioners have increasingly considered ways to prevent or otherwise address the negative effects of ACEs. For example, as of September 2017, 20 states had passed (or had pending) more than 40 bills that specifically mention ACEs, including legislation that establishes task forces to study ACEs and appropriation of funds for ACEs prevention.20,21 One challenge for such efforts is the diversity of experiences that fall under the umbrella of ACEs—from poverty to parental incarceration to community violence—which suggests that no single strategy will be adequate. States and localities address ACEs in a variety of ways that are often tailored to specific issues in local communities, and aimed at addressing multiple problems across sectors. For example, the state of Washington established the ACEs Public-Private Initiative, a collaborative of public agencies, private foundations, and community organizations dedicated to studying and implementing policies and practices that may prevent ACEs. An evaluation found promising positive outcomes in some communities, while noting that all community networks struggled to achieve community-wide change and that no single model worked best for developing the capacity to address ACEs and build resilience.22
While preventing the initial occurrence of ACEs is a logical priority, many children who have already experienced negative effects from ACEs have treatment needs. The American Academy of Pediatrics recommends that pediatricians regularly screen young children for circumstances (including maternal depression, parental substance abuse, poverty, and community violence) that can lead to toxic stress.23 If a child has experienced such adversities, health care providers can help the family address the immediate threat and reduce the likelihood of future exposure, and can make referrals to services and to evidence-based treatments that may mitigate the negative effects of the experience. However, the practice of screening for trauma, including ACEs, is not yet widespread among pediatricians.24 The evidence for intergenerational transmission of the effects of ACEs also argues for interventions that work simultaneously with parents and children.25
Conclusions
Despite increasing attention—and resources—devoted to preventing adverse childhood experiences and building resilient individuals and communities, ACEs remain common in the United States. Nearly half of all children nationally and in most states have experienced at least one ACE. It is difficult to generalize about the group of states in which children are more likely to have a high number of ACEs. However, among states highest on this measure, three (Arkansas, New Mexico, and Arizona) were among the ten states with the highest child poverty in 2016.35 More robust, multiyear data will be available in the future as ongoing surveying boosts sample sizes.
Disturbingly, black and Hispanic children and youth in almost all regions of the United States are more likely to experience ACEs than their white and Asian peers. To some extent, these racial disparities reflect the lasting effects of inequitable policies, practices, and social norms. Discriminatory housing and employment policies, bias in law enforcement and sentencing decisions, and immigration policies have concentrated disadvantage among black and Hispanic children, in particular, and leave them disproportionately vulnerable to traumatic experiences like ACEs.
Along with many other researchers, the study authors believe that the experience of racism can itself have toxic effects.36,37 It may be useful, as some researchers have done, to distinguish between catastrophic (acute) stressors and routine (chronic) ones,38 of which the experience of racism is an example. ACEs (including racism) can make people physically and mentally ill.39 Nevertheless, we believe that the NSCH item asking parents whether their child has been unfairly treated on the basis of race or ethnicity may not adequately assess the full extent—personal, institutional, and systemic—of children’s experience of racism. It may be challenging to accurately assess something with such pervasive (and historically embedded) effects that it may not even be remarked upon.40 There is a need to better understand how both adversity and resilience play out in diverse populations. For example, some evidence suggests that nativity status could be one important factor influencing the effects of ACEs. Hispanic children in immigrant families seem to be buffered from exposure to ACEs, relative to their peers with two U.S.-born parents.41
A number of researchers recommend expanding the concept of ACEs to include community-level stressors.42,43 These stressors may include unsafe neighborhoods, foster care arrangements, and bullying. Limiting surveys to household-level assessments of ACE exposure almost certainly results in underestimates.
The prospect of multigenerational effects stemming from the experience of childhood adversity underscores the urgency of applying a public-health approach to prevention. Such an approach would complement allied perspectives that address social determinants of health, and use intervention models that are explicitly two-generational: focusing simultaneously on the needs of adults (particularly parents) and children who have been exposed (or who are at risk of exposure) to ACEs. Fortunately, a growing number of programs show promise in this field.44 In addition, overdue attention is being given to protective or promotive factors—both of which fall within the concept of resilience.45,46 Adverse experiences do not necessarily lead to toxic levels of stress; here, the buffering role of social support and other protective factors is critical. The cultivation of supportive, protective conditions by parents, by children themselves, and by their broader communities provides an ambitious but essential public health agenda.
About the Data Used in This Brief
The National Survey of Children’s Health (NSCH) was conducted in 2003, 2007, 2011/12, and 2016 in all 50 states and the District of Columbia. The 2016 National Survey of Children’s Health was funded and directed by the Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB). The 2016 NSCH was significantly redesigned and differs from the prior survey cycles; therefore, comparisons cannot be drawn across all years of the survey. The survey uses an address-based sample that utilizes internet-based web and mailed paper data collection instruments fielded by the U.S. Census Bureau. One child in each household with children was randomly selected to be the focus of the study. A parent or guardian knowledgeable about the child answered questions about the child and themselves. The survey is representative of children under 18 years of age, both nationwide and within each state. A total of 50,212 surveys were completed.
The prevalence of ACEs described in this brief are derived from the following questions asked of parents:
- To the best of your knowledge, has this child EVER experienced any of the following?
- Parent or guardian divorced or separated (Yes/No)
- Parent or guardian died (Yes/No)
- Parent or guardian served time in jail (Yes/No)
- Saw or heard parents or adults slap, hit, kick, punch one another in the home (Yes/No)
- Was a victim of violence or witnessed violence in his or her neighborhood (Yes/No)
- Lived with anyone who was mentally ill, suicidal, or severely depressed (Yes/No)
- Lived with anyone who had a problem with alcohol or drugs (Yes/No)
- SINCE THIS CHILD WAS BORN, how often has it been very hard to get by on your family’s income—hard to cover the basics like food or housing? (Very Often, Somewhat Often, Rarely, Never)
Cases were not included in the analysis if any questions were left unanswered. Six percent of the sample did not answer any of the questions.
The relative confidence interval for each estimate presented in the tables is calculated by dividing the absolute 95 percent confidence interval by the estimate and multiplying by 100. If the relative confidence interval for a given estimate (for example, the percent of black non-Hispanic children with more than one ACE) is more than 120 percent, we suggest that the estimate be interpreted with caution, as it may not be reliable.
Differences between state and national estimates were tested for statistical significance by comparing the 95 percent confidence intervals. If the confidence intervals did not overlap, the differences are marked as significant in the tables.
Differences between the racial/ethnic groups were tested using an ordered logit regression, with white non-Hispanic as the reference group.
Included in the “Other, Non-Hispanic” category are children reported as Hawaiian/Pacific Islander, American Indian/Alaska Native, two or more races, or another race not already listed. For children in these racial categories, there were not sufficient numbers in the 2016 NSCH sample to allow reliable estimates of ACEs for all states or Census divisions.
References
1. Felitti, V. J., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245-258. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/9635069.
2. Sameroff, A., Gutman, L. M., & Peck, S. C. (2003). Adaptation among youth facing multiple risks: Prospective research findings. In S. S. Luthar, Ed., Resilience and vulnerability: Adaptation in the context of childhood adversities. Chapt. 15. (pp. 364–391). NY: Cambridge University Press.
3. U.S. Census Bureau. (undated). Geographic terms and concepts: Census divisions and census regions. Retrieved from https://www.census.gov/geo/reference/gtc/gtc_census_divreg.html.
4. Moore, K. A., & Ramirez, A. N. (2016). Adverse childhood experience and adolescent well-being: Do protective factors matter? Child Indicators Research, 9(2), 299-316. Retrieved from https://link.springer.com/article/10.1007/s12187-015-9324-4.
5. Bethell, C. D., Davis, M. B., Gombojav, N, Stumbo, S., & Powers, K. (2017). A national and across state profile on adverse childhood experiences among children and possibilities to heal and thrive. Retrieved from http://www.cahmi.org/projects/adverse-childhood-experiences-aces/.
6. Metzler, M., Merrick, M. T., Klevens, J., Ports, K. A., & Ford, D. C. (2017). Adverse childhood experiences and life opportunities: shifting the narrative. Children and Youth Services Review, 72, 141-149. Retrieved from http://www.sciencedirect.com/science/article/pii/S0190740916303449.
7. Bethell, C. D., Davis, MB, Gombojav, N, Stumbo, S, Powers, K. (2017). A national and across state profile on adverse childhood experiences among children and possibilities to heal and thrive. Retrieved from http://www.cahmi.org/projects/adverse-childhood-experiences-aces/.
8. Chartier, M. J., Walker, J. R., & Naimark, B. (2010). Separate and cumulative effects of adverse childhood experiences in predicting adult health and health care utilization. Child Abuse & Neglect, 34(6), 454-464. Retrieved from https://www.sciencedirect.com/science/article/pii/S0145213410000955.
9. Chapman, D.P., Whitfield, C.L., Felitti, V.J., Dube, S.R., Edwards, V.J, & Anda, R.F. (2004) Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82(2): 217-225. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15488250.
10. Felitti, V. J. et al. Op cit.
11. Rutter, M. (1979). Protective factors in children’s responses to stress and disadvantage. In M. Kent, & J. Rolf (Eds.), Primary prevention of psychopathology: III. Promoting social competence and coping in children (pp. 49–74). Hanover, NH: University Press of New England. Retrieved from http://europepmc.org/abstract/med/547874.
12. Mersky, J. P., Topitzes, J., & Reynolds, A. J. (2013). Impacts of adverse childhood experiences on health, mental health, and substance use in early adulthood: A cohort study of an urban, minority sample in the US. Child Abuse & Neglect, 37(11), 917-925. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4090696/.
13. Buss, C., Entringer, S., Moog, N. K., Toepfer, P., Fair, D. A., Simhan, H. N., & Wadhwa, P. D. (2017). Intergenerational transmission of maternal childhood maltreatment exposure: implications for fetal brain development. Journal of the American Academy of Child & Adolescent Psychiatry. 56(5). 373–382. Retrieved from http://www.jaacap.com/article/S0890-8567(17)30105-3/fulltext.
14. Monk, C., Feng, T., Lee, S., Krupska, I., Champagne, F. A., & Tycko, B. (2016). Distress during pregnancy: epigenetic regulation of placenta glucocorticoid-related genes and fetal neurobehavior. American Journal of Psychiatry, 173(7), 705-713. Retrieved from https://ajp.psychiatryonline.org/doi/abs/10.1176/appi.ajp.2015.15091171.
15. Almond, D., & Currie, J. (2011). Killing me softly: The fetal origins hypothesis. The Journal of Economic Perspectives, 25(3), 153-172. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4140221/pdf/nihms443660.pdf.
16. Madigan, S., Wade, M., Plamondon, A., Maguire, J. L., & Jenkins, J. M. (2017). Maternal Adverse Childhood Experience and Infant Health: Biomedical and Psychosocial Risks as Intermediary Mechanisms. The Journal of Pediatrics, 187, 282-289.e1. Retrieved from http://www.sciencedirect.com/science/article/pii/S0022347617305991
17. Felitti, V. J. et al. Op cit.
18. Bethell, C. D., Carle, A., Hudziak, J., Gombojav, N., Powers, K., Wade, R., & Braveman, P. (2017). Methods to assess adverse childhood experiences of children and families: toward approaches to promote child well-being in policy and practice. Academic Pediatrics, 17(7), S51-S69. Retrieved from http://www.academicpedsjnl.net/article/S1876-2859(17)30324-8/abstract.
19. Substance Abuse and Mental Health Services Administration. (2014). Trauma-informed care in behavioral health services: A treatment improvement protocol. Retrieved from https://www.integration.samhsa.gov/clinical-practice/SAMSA_TIP_Trauma.pdf.
20. NCSL Health Program Staff. (2017). Ten Key State Issues in Public Health (Blog post). National Conference of State Legislatures. Retrieved from http://www.ncsl.org/blog/2017/09/28/ten-key-state-issues-in-public-health-part-2.aspx.
21. Prewitt, E. (2017). Update on Bumper Crop of State ACEs bills in 2017—46 bills in 20 states (Blog post). States ACEs Action. Retrieved from http://www.acesconnection.com/g/state-aces-action-group/blog/update-on-bumper-crop-of-state-aces-bills-in-2017-46-bills-in-20-states.
22. Verbitsky-Savitz, N., Hargreaves, M., Penoyer, S., Morales, N., Coffee-Borden, B., & Whitesell, E. (2016). Preventing and Mitigating the Effects of ACEs by Building Community Capacity and Resilience: APPI Cross-Site Evaluation Findings. Mathematica Policy Research. Retrieved from https://www.mathematica-mpr.com/our-publications-and-findings/publications/final-report-preventing-and-mitigating-the-effects-of-aces-by-building-community-capacity.
23. American Academy of Pediatrics. (2017). American Academy of Pediatrics Recommends Pediatricians Screen for Poverty at Check-ups and Help Eliminate its Toxic Health Effects. Retrieved from https://www.aap.org/en-us/Documents/journals_research_update.pdf and https://www.aap.org/en-us/about-the-aap/aap-press-room/Pages/American-Academy-of-Pediatrics-Recommends-Pediatricians-Screen-for-Poverty-at-Check-ups-and-Help-Eliminate-its-Toxic-Health.aspx.
24. Kerker, B. D., Storfer-Isser, A., Szilagyi, M., Stein, R. E., Garner, A. S., O’Connor, K. G., & Horwitz, S. M. (2016). Do pediatricians ask about adverse childhood experiences in pediatric primary care? Academic Pediatrics, 16(2), 154-160.
25. Sun, J., Patel, F., Rose-Jacobs, R., Frank, D.A., Black, M.M., Chilton, M. (2017). Mother’s adverse childhood experiences and their young children’s development. American Journal of Preventive Medicine, 53(6), 882-891. Retrieved from: http://www.ajpmonline.org/article/S0749-3797(17)30422-1/pdf.
26. Moore, K. A., & Ramirez, A. N. (2016). Adverse childhood experience and adolescent well-being: Do protective factors matter?. Child Indicators Research, 9(2), 299-316. Retrieved from https://www.aap.org/en-us/Documents/journals_research_update.pdf.
27. Sege, R., Bethell, C., Linkenbach, J., Jones, J.A., Klika, B., Pecora, P.J. (2017). Balancing adverse childhood experiences (ACEs) with HOPE*: New insights into the role of positive experience on child and family development. Casey Family Programs. Retrieved from https://www.cssp.org/publications/documents/Balancing-ACEs-with-HOPE-FINAL.pdf.
28. Shonkoff, J. P., Boyce, W. T., Cameron, J., Duncan, G. J., Fox, N. A., Gunnar, M. R., & Thompson, R. A. (2005). Excessive stress disrupts the architecture of the developing brain. National Scientific Council on the Developing Child, Working Paper, 3, 2014. Retrieved from http://developingchild.harvard.edu/wp-content/uploads/2005/05/Stress_Disrupts_Architecture_Developing_Brain-1.pdf.
29. Bethell, C. D., Newacheck, P., Hawes, E., & Halfon, N. (2014). Adverse childhood experiences: assessing the impact on health and school engagement and the mitigating role of resilience. Health Affairs, 33(12), 2106-2115. Retrieved from https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.2014.0914.
30. American Psychological Assiciation. (2017). Resilience guide for parents & teachers. Retrieved from http://www.apa.org/helpcenter/resilience.aspx.
31. Substance Abuse and Mental Health Services Administration. (2017). Trauma-informed approach and trauma-specific interventions. Retrieved from https://www.samhsa.gov/nctic/trauma-interventions.
32. Bartlett, D.J., Wilson, A., Moore, K.A., & Redd, Z. (2016). 5 ways trauma-informed care supports children’s development. Child Trends: Bethesda, MD. Retrieved from https://www.childtrends.org/publications/5-ways-trauma-informed-care-supports-childrens-development.
33. Bartlett, D.J., Smith, S., & Bringewatt, E. (2017). Helping young children who have experienced trauma: Policies and strategies for early care and education. Child Trends: Bethesda, MD. Retrieved from https://www.childtrends.org/publications/ecetrauma/.
34. Murphy, K., Moore, Kristin A., Redd, Z., Malm, K. (2017). Trauma-informed child welfare systems and children’s well-being: A longitudinal evaluation of KVC’s bridging the way home initiative. Children and Youth Services Review, 70, 23-34. https://www.sciencedirect.com/science/article/pii/S0190740917301342
35. The Annie E. Casey Foundation, KIDS COUNT Data Center. (2017). The Annie E. Casey Foundation. Retrieved from http://datacenter.kidscount.org/data/tables/65-median-family-income-among-households-with-children?loc=1&loct=2#ranking/2/any/true/870/any/365.
36. Huynh, V. W., Guan, S.-S. A., Almeida, D. M., McCreath, H., & Fuligni, A. J. (2016). Everyday Discrimination and Diurnal Cortisol during Adolescence. Hormones and Behavior, 80, 76–81. http://doi.org/10.1016/j.yhbeh.2016.01.009/; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4409660/.
37. Brody, G. H., Yu, T., Miller, G. E., & Chen, E. (2015). Discrimination, Racial Identity, and Cytokine Levels Among African American Adolescents. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 56(5), 496–501. http://doi.org/10.1016/j.jadohealth.2015.01.017.
38. Odgers, C. L., & Jaffee, S. R. (2013). Routine versus catastrophic influences on the developing child. Annual Review of Public Health, 34, 29-48. Retrieved from http://www.annualreviews.org/doi/abs/10.1146/annurev-publhealth-031912-114447.
39. Priest, N., Paradies, Y., Trenerry, B., Truong, M., Karlsen, S., & Kelly, Y. (2013). A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine, 95, 115-127. Retrieved from http://www.sciencedirect.com/science/article/pii/S0277953612007927.
40. Wade, R., Shea, J. A., Rubin, D., & Wood, J. (2014). Adverse childhood experiences of low-income urban youth. Pediatrics, 134(1), e13-e20. Retrieved from http://pediatrics.aappublications.org/content/134/1/e13.short.
41. Caballero, T. M., Johnson, S. B., Buchanan, C. R. M., & DeCamp, L. R. (2017). Adverse Childhood Experiences Among Hispanic Children in Immigrant Families Versus US-Native Families. Pediatrics, 140(5), e20170297. Retrieved from http://pediatrics.aappublications.org/content/140/5/e20170297.
42. Cronholm, P.F., Forke, C.M, Wade, R., Bair-Merritt, M.H., Davis, M., Harkins-Schwarz, M., Pachter, L.M., Fein, J.A., (2015). Adverse Childhood Experiences Expanding the Concept of Adversity. American Journal of Preventive Medicine, 49(3), 354-361. Retrieved from: http://www.ajpmonline.org/article/S0749-3797(15)00050-1/pdf.
43. Bruner, C. (2017). ACE, Place, Race, and Poverty: Building Hope for Children. Community and Family Approaches, 17(7S), S123-S129. Retrieved from: http://www.academicpedsjnl.net/article/S1876-2859(17)30352-2/pdf.
44. Bartlett, Dym J., Smith, S., & Bringewatt, E. (2017). Helping young children who have experienced trauma: Policies and strategies for early care and education. Child Trends: Bethesda, MD. Retrieved from https://childtrends-ciw49tixgw5lbab.stackpathdns.com/wp-content/uploads/2017/04/2017-19ECETrauma.pdf.
45. Traub, F., & Boynton-Jarrett, R. (2017). Modifiable Resilience Factors to Childhood Adversity for Clinical Pediatric Practice. Pediatrics, e20162569. Retrieved from http://pediatrics.aappublications.org/content/early/2017/04/17/peds.2016-2569.
46. Traub, F. E. (2016). Factors for improving short-and long-term health outcomes for children who have experienced adversity and trauma (Doctoral dissertation). Retrieved from https://open.bu.edu/bitstream/handle/2144/19471/Traub_bu_0017N_12325.pdf?sequence=1.
This research was funded by the Annie E. Casey Foundation. We thank them for their support but acknowledge that the findings and conclusions presented in this report are those of the authors alone, and do not necessarily reflect the opinions of the Foundation. We would also like to thank Jessica Dym Bartlett, Maria A. Ramos-Olazagasti, Kristine Andrews, and Kristin Moore for their review.